The Analytics of “Lyme disease” & RICO evidence database –
Blog File created Sept 20th, 2017, links are live.
Background: We should always start with the fact that OspA as a triacyl lipoprotein could never have been a vaccine, so, see for yourself:
https://www.ncbi.nlm.nih.gov/pubmed/?term=(pam3cys+or+Pam3*+or+P3C*+or+lipoprotein)+and+tlr2+and+tlr1
.
“Typically, lipoproteins are tri-acylated in Gram-negative bacteria and di-acylated in Gram-positive bacteria and Mycobacterium 8, 9. The canonical triacyl form is proposed to be recognized by TLR1/2, and the diacyl form by TLR2/6 10. ”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5553087/
That which is a 3-acyl lipoprotein is a TLR2/1 agonist (like the OspA Lyme vaccine or any new fake one with pam3cys on it) and is a fungal endotoxin, and never could be a “vaccine,” period. Fungal endotoxins cause sepsis then immunosuppression.
The latest “Lyme vaccine” has Pam3Cys on it. Someone did not get the memo:

http://news.bioscholar.com/2014/11/researchers-developed-vaccine-prevent-lyme-disease.html
The Lyme criminals (ALDF.com founded by CDC officers, mainly Alan Barbour, Allen Steere, and Barbara Johnson) said, criminally, basically, “the more the antibodies, that makes the test the more betterer”:
.
“Band intensity analysis increases the objectivity and accuracy of Western blot interpretation for the diagnosis of Lyme arthritis.” — Lyme criminal Arthur Weinstein
https://www.ncbi.nlm.nih.gov/pubmed/8053960
False. RIDIC-a-RICO. This is the equivalent of saying, “Alligators may only be called alligators if they are 12 feet long. Anything less is not an alligator, it is some other creature.” We know alligators by their SPECIFIC FEATURES (like skin, jaws, tail, scary pointy clawed feet, etc). And if there any running around in your house, no matter how long, you’d want to know. It’s hard for us to believe we have never seen anyone with “MD” after their names complain about Crazy Allen Steere’s proposal for how to detect a disease, but that’s true. We haven’t.
One tries to imagine what medical school is like. “Run this test, Run that test, Give this drug, Give that drug,” but they never get the why’s or the history. They must be exposed to narrow pockets of information and one thing is never shown to be related to another. We have oncology and rheumatology but we never find an oncologist who knows lymphoma is related to EBV or that there is an association between ALS and fungal antigens (like LYMErix or the OspA Lyme vaccines):
https://www.ncbi.nlm.nih.gov/pubmed/?term=als+and+fung*
A one Holly Ahern of SUNY (Adirondack? a lab instructor?) told me on the phone that Multiple Sclerosis was not caused by EBV-and-The-Boys and that there was no literature to support such a claim, and I had to reply, “Do you know how to use PubMed?” Whereupon, she hung up on me. She claims to know about Lyme disease, but she has never heard, apparently, that Lyme causes MS, even according to the NIH who until recently has a special division under the NINDS.gov that dealt with “How Lyme Causes MS (via reactivation of EBV),” just like Yale had a “Lyme and Lupus Clinic.”
Yikes.
“If you hear hoofbeats behind you, think horses not zebras.” If Lyme causes, well, everything, well, what causes everything? Immunosuppression and the reactivation of Our Friends, The Latent Herpesviruses. The Judys and the Hollys of this world? Oy. I wish they would shut up and do their homework. I wonder if they could be court-ordered to learn how to use PubMed. ‘Same for all the “MDs” out there. It’s an epidemic of virtual ignorance. The more access we have to information, the less most of us use it. Why do I even have this blog 18 years after the fact. Borrelia gimmeabreakii.
All the BASIC SCIENCE seems to be handed over by default to the victims of these MD-tards and their BigPharma or BigInsurance pimps. Thanks. What does “medical” or “doctor” even mean any more. How can anyone have a PhD in a medical science and never ask what the thing is, either?
The Main ComplaintS – plural, but they mean the same thing:
The main complaint we have regarding the Cabal (ALDF.com) is that they falsified the testing at Dearborn (MI, 1994) such as to make their fake vaccine, OspA, appear “safe and effective” when it fact, it, as a fungal triacyl-lipoprotein, gave the victims the same fungal endotoxin “sepsis-induced immunosuppression” response that we call “Chronic Neurologic Lyme (it’s really about EBV and The Boys).”
Therefore, fixing the Lyme testing crime alone will not fix the problem. Fixing the testing alone will just create more opportunities for the ever-growing class of charlatans who think Lyme can be treated with antibiotics (how so, when it is viral and like AIDS, with a B cell disorder?), or the Rifing or Onion Socks or Carrot Juice/Diet Voodoo. (Puh-lease.)
The consensus of the “participating” labs at the 1994 Dearborn conference on average stated that the new (research fraud, Steere) proposal for a two tiered testing method that required the ELISA to screen out anything that was not hypersensitivity or allergy or autoimmune monoarthritis-in-a-knee Lyme, and then on to the blot to look for “too many specific antibodies,” … was 15% accurate or detected only 15% of the “cases.” You can see this difference clearly in the comparison of the Western Blots shown in the racketeering case filed against these criminals with justice.gov.
This is page 3 of that 2003 complaint:

The ALDF.com Lyme criminals including patent-holding CDC officers changed the testing because their vaccine caused the same disease, which means the vaccine caused the same disease, which means this disease is not about spirochetes. It is about post-endotoxin sepsis caused by the shed Osps (or Vmps, or Vsps, or Omps,or Tmps depending on the spirochete genera we are talking about), which are fungal (triacyl-lipoproteins, TLR2/1 agonists). The “Great Imitator” is really Epstein-Barr and the like. And nothing is really “autoimmune” anything, it seems:
J Exp Med. 1996 Mar 1;183(3):1161-72.
B lymphocytes secrete antigen-presenting vesicles.
Raposo G1, Nijman HW, Stoorvogel W, Liejendekker R, Harding CV, Melief CJ, Geuze HJ.
Antigen-presenting cells contain a specialized late endocytic compartment, MIIC (major histocompatibility complex [MHC] class II-enriched compartment), that harbors newly synthesized MHC class II molecules in transit to the plasma membrane. MIICs have a limiting membrane enclosing characteristic internal membrane vesicles. Both the limiting membrane and the internal vesicles contain MHC class II. In this study on B lymphoblastoid cells, we demonstrate by immunoelectron microscopy that the limiting membrane of MIICs can fuse directly with the plasma membrane, resulting in release from the cells of internal MHC class II-containing vesicles. These secreted vesicles, named exosomes, were isolated from the cell culture media by differential centrifugation followed by flotation on sucrose density gradients. The overall surface protein composition of exosomes differed significantly from that of the plasma membrane. Exosome-bound MHC class II was in a compact, peptide-bound conformation. Metabolically labeled MHC class II was released into the extracellular medium with relatively slow kinetics, 10 +/- 4% in 24 h, indicating that direct fusion of MIICs with the plasma membrane is not the major pathway by which MHC class II reaches the plasma membrane. Exosomes derived from both human and murine B lymphocytes induced antigen-specific MHC class II-restricted T cell responses. These data suggest a role for exosomes in antigen presentation in vivo.
https://www.ncbi.nlm.nih.gov/pubmed/8642258
The above article by CV Harding was cited by over 500 other articles:
https://www.ncbi.nlm.nih.gov/pubmed?linkname=pubmed_pubmed_citedin&from_uid=8642258
We think this debunks all of Allen Steere’s theories about what is happening in his Autoimmune-Bad-Knees, too. The antigen must still be there.
J Autoimmun. 2001 May;16(3):263-8.
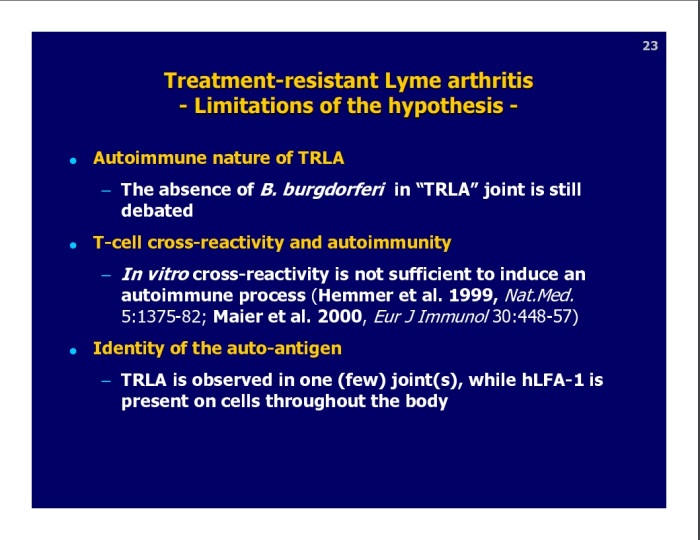
Autoimmune mechanisms in antibiotic treatment-resistant lyme arthritis.
Steere AC1, Gross D, Meyer AL, Huber BT.
In about 10% of patients with Lyme arthritis in the United States, joint inflammation persists for months or even several years after the apparent eradication of the spirochete, Borrelia burgdorferi, from the joint with antibiotic treatment. We propose a model of molecular mimicry affecting genetically susceptible individuals to explain this treatment-resistant course. The majority of patients with treatment-resistant Lymearthritis have HLA-DRB1*0401 or related alleles, and the severity and duration of their arthritis correlate with cellular and humoral immune responses to outer-surface protein A OspA) of the spirochete. Using an algorithm, the immunodominant epitope of OspA presented by the DRB1*0401 molecule was predicted to be located at aa 165-173. In a search of the Genetics Computer Group gene bank, only one human protein was identified, lymphocyte function associated antigen-1 (hLFA-1), that had sequence homology with OspA(165-173)and predicted binding in the DRB1*0401 molecule. Synovial fluid T cells from most patients with treatment-resistant arthritis responded to both OspA and hLFA-1, whereas those from patients with other forms of chronic inflammatory arthritis did not. Molecular mimicry between a dominant T cell epitope of OspA and hLFA-1 may be an important factor in the persistence of joint inflammation in genetically susceptible patients with treatment-resistant Lyme arthritis.
https://www.ncbi.nlm.nih.gov/pubmed/11334491
The latest on that (2016, Clifford Harding again); you’ll want to read the entire report.
“Contributions of extracellular vesicles to immune evasion.
“Exosomes and other ExMVs have been implicated in the pathogenesis of many different viruses (Figure 1). Upon release, these vesicles are “captured” by cells, and the transfer of host and viral proteins and/or RNA could enhance viral infection and replication in recipient cells, or inhibit the immune response through induction of apoptosis or by blocking key cellular responses. In the case of human CMV, microvesicles released by infected cells contain soluble DC-SIGN, a C-type lectin family molecule, in complex with CMV glycoprotein B. Release of this complex through microvesicles and its interaction with target cells appears to increase the susceptibility of recipient cells to CMV infection (47). Similarly, in HCV-infected patients, the interaction of the cellular membrane protein CD81 with HCV envelope glycoprotein E2 and the release of this complex within microvesicles and subsequent interaction with recipient cells increase the susceptibility of recipient cells to HCV (48). Exosomes and other ExMVs released from HIV-1–infected peripheral blood mononuclear cells (PBMCs) or from megakaryocytes and platelets contain CCR5 and CXCR4, respectively. In both cases, the transfer of these chemokine receptors to target cells enhances their susceptibility to HIV infection (49, 50). Work by Campbell and colleagues showed that Nef is present in exosomes secreted from transfected HEK 293 cells, which, upon fusion with uninfected Jurkat T cells, restore infectivity to Nef-negative HIV virions (31). Together, these results suggest that ExMVs released during viral infections enhance the infectivity of neighboring cells, preparing the way for the soon-to-be-released viral particles.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4811125/
.
SmithKline’s Yves Lobet debunked Steere’s Theory at the January 2001 FDA Hearing on LYMErix adverse events by saying…
https://www.fda.gov/ohrms/dockets/ac/01/slides/3680s2_02_lobet.pdf
SmithKline said, to the FDA, that if this thing that Steere claims is the cause of autoimmune bad knees is real, then why does this occur only in knees or other single joints if hFLA-a is “present on cells throughout the body?” It must be because the antigen or the bug is still there, meaning there is no such thing as autoimmune bad knees. Could it be ongoing shedding of the lipoproteins and perhaps the antigen with its HLA complex attached (as a kind of exosome) that creates a new antigen (as a complex)? All we know for sure about Steere and his crazy theories of Autoimmune Bad-Knee-Lyme is that he has never found out or reported how exactly his proposal works in the last 42 years. ‘Famous for never discovering anything or letting go of a failed, fraudulent unscientific theory. Cheers. Let’s name a day after him like Columbus Day.
We showed in the truthcures.org charge sheets that the NIH and others know and have reported that these shed antigens circulate to the brain and inflame it (chronically).
An NIH patent, explaining how Lyme causes LYMErix-disease:
“The invention relates to novel antigens associated with Borrelia burgdorferi which are exported (or shed) in vivo and whose detection is a means of diagnosing Lyme disease. The antigens are extracellular membrane vesicles and other bioproducts including the major extracellular protein antigen. Another object of the invention is to provide antibodies, monoclonal and/or polyclonal, labeled and/or unlabeled, that are raised against the antigens. A further object of the invention is to provide a method of diagnosing Lyme disease by detecting the antigens in a biological sample taken from a host using the antibodies in conventional immunoassay formats. Another object of the invention is to provide kits, for the diagnosis of Lyme disease, comprising the antibodies and ancillary reagents. The advantage of the antibodies used in the invention is that they react with the antigens from geographically diverse strains of Borrelia burgdorferi, but do not react with antigens from related Borrelia spirochetes.”
http://patft.uspto.gov/netacgi/nph-Parser?Sect1=PTO1&Sect2=HITOFF&d=PALL&p=1&u=%2Fnetahtml%2FPTO%2Fsrchnum.htm&r=1&f=G&l=50&s1=5,217,872.PN.&OS=PN/5,217,872&RS=PN/5,217,872
AAAAaaaand…
Characterization of multiprotein complexes of the Borrelia burgdorferi outer membrane vesicles.
“Although we uncovered the existence of at least 10 distinct OM complexes harboring several unique subunits, the complexome is dominated by the frequent occurrence of a limited diversity of membrane proteins, most notably P13, outer surface protein (Osp) A, -B, -C, and -D and Lp6.6.”
http://www.ncbi.nlm.nih.gov/pubmed/21875077
AAAAaaaand…
Am J Pathol. 2010 Jun;176(6):2848-57. doi: 10.2353/ajpath.2010.091235. Epub 2010 Apr 29.
Bacterial lipoproteins can disseminate from the periphery to inflame the brain.
Londoño D1, Cadavid D.
The current view is that bacteria need to enter the brain to cause inflammation. However, in mice infected with the spirochete Borreliaturicatae, we observed widespread cerebral inflammation despite a paucity of spirochetes in the brain parenchyma at times of high bacteremia. Here we studied the possibility that bacterial lipoproteins may be capable of disseminating from the periphery across the blood-brain barrier to inflame the brain. For this we injected normal and infected mice intraperitoneally with lanthanide-labeled variable outer membrane lipoproteins of B. turicatae and measured their localization in blood, various peripheral organs, and whole and capillary-depleted brain protein extracts at various times. Lanthanide-labeled nonlipidated lipoproteins of B. turicatae and mouse albumin were used as controls. Brain inflammation was measured by TaqMan RT-PCR amplification of genes known to be up-regulated in response to borrelial infection. The results showed that the two lipoproteins we studied, LVsp1 and LVsp2, were capable of inflaming the brain after intraperitoneal injection to different degrees: LVsp1 was better than LVsp2 and Bt1 spirochetes at moving from blood to brain. The dissemination of LVsp1 from the periphery to the brain occurred under normal conditions and significantly increased with infection. In contrast, LVsp2 disseminated better to peripheral organs. We conclude that some bacterial lipoproteins can disseminate from the periphery to inflame the brain.
https://www.ncbi.nlm.nih.gov/pubmed/20431027
BAUMGARTH – COMPARE to HARDING and Radolf on fungal lipoproteins inhibiting antigen-presentation or HLA handling of the antigen, and how he says this is the reason for the no-antibody production,
“Thus, it is of interest to consider potential roles for the inhibition of the CP beyond protection from complement-mediated attack. For example, upon colonizing lymph tissue B. burgdorferi disrupts the normal formation of germinal centers (GC) [60,61]. Lack of normal GC development ultimately results in reduced antibody titers against B. burgdorferi in experimental infection [60]. Local complement C4 deposition on follicular dendritic cells (FDC) is significantly reduced in B. burgdorferi infected lymph nodes and this is speculated to be responsible for the premature collapse of GC responses due to diminished antigen presentation by FDCs [60].”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4725857/#ppat.1005404.ref060
Again….
“Local complement C4 deposition on follicular dendritic cells (FDC) is significantly reduced in B. burgdorferi infected lymph nodes and ***this is speculated to be responsible for the premature collapse of GC responses due to diminished antigen presentation by FDCs ***…”
Here is what Baumgarth said, most recently:
“By decreasing the capacity of the host to produce effective antibodies against B. burgdorferi, the GC collapse may help B. burgdorferi evade clearance. The signals and mechanisms leading to the collapse, however, are unknown. One possible mechanism is the interference of B. burgdorferi with the complement system. Continued antigen presentation is crucial for hyperaffinity maturation, and components of the complement system are known to be involved in this process. Specifically, activated C3 and C4 fragments bound to antigen and adhere to complement receptors 1 and 2 (CR1 and CR2). These receptors are present on the major antigen-presenting cells in the GC, the FDC, and on GC B cells. It was shown previously that GCs will form normally in mice lacking CR1 and CR2, but collapse prematurely, before GCs can perform their important functions (120). This phenotype is strikingly similar to that seen in wild-type mice infected with B. burgdorferi. Interestingly, in B. burgdorferi-infected mice, although CR1 and CR2 are present on FDCs and GC B cells, C4 is not detectable (69). C4 is typically deposited on the surface of FDCs supporting antigen presentation. Interference with C4 deposition could inhibit antigen presentation by FDCs to GC B cells and thereby lead to GC collapse. B. burgdorferi interference with activation of complement could also have various indirect effects on GCs: changing the cytokine milieu, reducing antigen presentation to naïve B cells via CR1 on APCs outside the GC, reducing naïve B cell activation viaco-stimulation with CR2, and reducing opsonization (and thus uptake) of antigens. Exploring the role of complement and complement inhibition by B. burgdorferi during infection are important subjects for future studies.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5316537/
Of course there is another reason antigen is not presented – it could be OspA, or Pam3Cys, which downregulates that function, meaning no antibodies will be produced:
Harding and Radolf:
J Immunol. 2001 Jul 15;167(2):910-8.
Toll-like receptor 2-dependent inhibition of macrophage class II MHC expression and antigen processing by 19-kDa lipoprotein of Mycobacterium tuberculosis.
Noss EH1, Pai RK, Sellati TJ, Radolf JD, Belisle J, Golenbock DT, Boom WH, Harding CV.
Mycobacterium tuberculosis (MTB) induces vigorous immune responses, yet persists inside macrophages, evading host immunity. MTB bacilli or lysate was found to inhibit macrophage expression of class II MHC (MHC-II) molecules and MHC-II Ag processing. This report characterizes and identifies a specific component of MTB that mediates these inhibitory effects. The inhibitor was extracted from MTB lysate with Triton X-114, isolated by gel electroelution, and identified with Abs to be MTB 19-kDa lipoprotein. Electroelution- or immunoaffinity-purified MTB 19-kDa lipoprotein inhibited MHC-II expression and processing of both soluble Ags and Ag 85B from intact MTB bacilli. Inhibition of MHC-II Ag processing by either MTB bacilli or purified MTB 19-kDa lipoprotein was dependent on Toll-like receptor (TLR) 2 and independent of TLR 4. Synthetic analogs of lipopeptides from Treponema pallidum also inhibited Ag processing. Despite the ability of MTB 19-kDa lipoprotein to activate microbicidal and innate immune functions early in infection, TLR 2-dependent inhibition of MHC-II expression and Ag processing by MTB 19-kDa lipoprotein during later phases of macrophage infection may prevent presentation of MTB Ags and decrease recognition by T cells. This mechanism may allow intracellular MTB to evade immune surveillance and maintain chronic infection.
https://www.ncbi.nlm.nih.gov/pubmed/?term=harding+and+radolf
AAAaaand…
J Immunol. 2005 Jun 1;174(11):6639-47.
Role of TLR in B cell development: signaling through TLR4 promotes B cell maturation and is inhibited by TLR2.
Hayashi EA1, Akira S, Nobrega A.
The role of TLR4 in mature B cell activation is well characterized. However, little is known about TLR4 role in B cell development. Here, we analyzed the effects of TLR4 and TLR2 agonists on B cell development using an in vitro model of B cell maturation. Highly purified B220(+)IgM(-) B cell precursors from normal C57BL/6 mouse were cultured for 72 h, and B cell maturation in the presence of the TLR agonists was evaluated by expression of IgM, IgD, CD23, and AA4. The addition of LPS or lipid A resulted in a marked increase in the percentage of CD23(+) B cells, while Pam3Cys had no effect alone, but inhibited the increase of CD23(+) B cell population induced by lipid A or LPS. The TLR4-induced expression of CD23 is not accompanied by full activation of the lymphocyte, as suggested by the absence of activation Ag CD69. Experiments with TLR2-knockout mice confirmed that the inhibitory effects of Pam3Cys depend on the expression of TLR2. We studied the effects of TLR-agonists on early steps of B cell differentiation by analyzing IL-7 responsiveness and phenotype of early B cell precursors: we found that both lipid A and Pam3Cys impaired IL-7-dependent proliferation; however, while lipid A up-regulates B220 surface marker, consistent with a more mature phenotype of the IgM(-) precursors, Pam3Cys keeps the precursors on a more immature stage. Taken together, our results suggest that TLR4 signaling favors B lymphocyte maturation, whereas TLR2 arrests/retards that process, ascribing new roles for TLRs in B cell physiology.
https://www.ncbi.nlm.nih.gov/pubmed/15905502
For those of you who dont know, Justin Radolf is one of the Lyme criminals.
Pam3Cys or OspA or the fungal antigens shed by spirochetes seem to be the source of the destroyed immune system that results in an AIDS-like (Acquired Immune Deficiency, not HIV) disease. Whoever cant explain and show these facts and this science, should never charge you a cent for any kind of treatment unless these treatments address this science and this physiology and Steere’s famous Deformed B Cells that look pre-cancerous.
“LLMDs” or ILADS.org treatments for “Lyme” and “Coinfections” has failed for the last 17+ years, but they also refuse to let go of their unscientific model.
The new news on that topic is this (Oct, 2017):
Biomaterials. 2017 Oct;142:1-12. doi: 10.1016/j.biomaterials.2017.07.011. Epub 2017 Jul 10.
Macrophage exosomes as natural nanocarriers for protein delivery to inflamed brain.
Yuan D1, Zhao Y1, Banks WA2, Bullock KM3, Haney M1, Batrakova E1, Kabanov AV4.
Recent work has stimulated interest in the use of exosomes as nanocarriers for delivery of small drugs, RNAs, and proteins to the central nervous system (CNS). To overcome the blood-brain barrier (BBB), exosomes were modified with brain homing peptides that target brain endothelium but likely to increase immune response. Here for the first time we demonstrate that there is no need for such modification to penetrate the BBB in mammals. The naïve macrophage (Mϕ) exosomes can utilize, 1) on the one hand, the integrin lymphocyte function-associated antigen 1 (LFA-1)*** [?Steere?] and intercellular adhesion molecule 1 (ICAM-1), and, 2) on the other hand, the carbohydrate-binding C-type lectin receptors, to interact with brain microvessel endothelial cells comprising the BBB. Notably, upregulation of ICAM-1, a common process in inflammation, promotes Mϕ exosomes uptake in the BBB cells. We further demonstrate in vivo that naïve Mϕ exosomes, after intravenous (IV) administration, cross the BBB and deliver a cargo protein, the brain derived neurotrophic factor (BDNF), to the brain. This delivery is enhanced in the presence of brain inflammation, a condition often present in CNS diseases. Taken together, the findings are of interest to basic science and possible use of Mϕ-derived exosomes as nanocarriers for brain delivery of therapeutic proteins to treat CNS diseases.
https://www.ncbi.nlm.nih.gov/pubmed/28715655
^^^Once again, it seems possible the so called “autoimmune” bad-knee-Lyme refers to something on the blebs ??
And here is the NIH >>>> saying Lyme and LYMErix disease are due to the shed blebs or the Borrelial Osp-ish-bearing exosomes causing humoral (in the body or blood samples) immunosuppression, but with chronic brain inflammation:
J Neuropathol Exp Neurol. 2006 Jun;65(6):540-8.
Borrelia burgdorferi Induces TLR1 and TLR2 in human microglia and peripheral blood monocytes but differentially regulates HLA-class II expression.
Cassiani-Ingoni R1, Cabral ES, Lünemann JD, Garza Z, Magnus T, Gelderblom H, Munson PJ, Marques A, Martin R.
The spirochete Borrelia burgdorferi is the agent of Lyme disease, which causes central nervous system manifestations in up to 20% of patients. We investigated the response of human brain microglial cells, glial progenitors, neurons, astrocytes, as well as peripheral blood monocytes to stimulation with B. burgdorferi. We used oligoarrays to detect changes in the expression of genes important for shaping adaptive and innate immune responses. We found that stimulation with B. burgdorferi lysate increased the expression of Toll-like receptors (TLRs) 1 and 2 in all cell types except neurons. However, despite similarities in global gene profiles of monocytes and microglia, only microglial cells responded to the stimulation with a robust increase in HLA-DR, HLA-DQ, and also coexpressed CD11-c, a dendritic cell marker. In contrast, a large number of HLA-related molecules were repressed at both the RNA and the protein levels in stimulated monocytes, whereas secretion of IL-10 and TNF-alpha was strongly induced. These results show that signaling through TLR1/2 in response to B. burgdorferi can elicit opposite immunoregulatory effects in blood and in brain immune cells, which could play a role in the different susceptibility of these compartments to infection.
https://www.ncbi.nlm.nih.gov/pubmed/16783164
And here is the NIH >>>> saying that due to the fungal shed Osps (or whatever you want to call the fungal, TLR2/1 agonist triacyl lipopeptides of spirochetes, since this is not limited to B. burgdorferi), you might not even have TLR5 (flagellin) agonist responses or band 41 on a Lyme Western Blot:
J Infect Dis. 2006 Mar 15;193(6):849-59. Epub 2006 Feb 8.
Borrelia burgdorferi lipoprotein-mediated TLR2 stimulation causes the down-regulation of TLR5 in human monocytes.
Cabral ES1, Gelderblom H, Hornung RL, Munson PJ, Martin R, Marques AR.
Toll-like receptors (TLRs) trigger innate immune responses via the recognition of conserved pathogen-associated molecular patterns. Lipoproteins from Borrelia burgdorferi, the agent of Lyme disease, activate inflammatory cells through TLR2 and TLR1. We show that stimulation of human monocytes with B. burgdorferi lysate, lipidated outer surface protein A, and triacylated lipopeptide Pam3CysSerLys4 results in the up-regulation of both TLR2 and TLR1 but the down-regulation of TLR5, the receptor for bacterial flagellin, and that this effect is mediated via TLR2. TLR4 stimulation had no effect on TLR2, TLR1, and TLR5 expression. Human monocytes stimulated with TLR5 ligands (including p37 or flaA, the minor protein from B. burgdorferi flagella) up-regulated TLR5. In addition, TLR2 stimulation rendered cells hyporesponsive to a TLR5 agonist. These results indicate that diverse stimuli can cause differential TLR expression, and we hypothesize that these changes may be useful for either the pathogen and/or the host.
https://www.ncbi.nlm.nih.gov/pubmed/16479520
So, here you have just seen the NIH agrees that Lyme or Borreliosis can be completely seronegative (no antibodies at all, not just only band 41 or the anti-flagelllar antibody) due to the fact of LYMErix, or the shed blebs or exosomes of Borreliae (with an “e” on the end refers to the entire genus) having the likes of the Osps/Vmps on them, cause tolerance and cross tolerance (no more responses by the body to other antigen types besides lipoproteins), but with chronic brain inflammation, and that,… Lyme is not “an autoimmune bad knee with too many antibodies” making the current CDC “case definition” – as shown in the DOJ RICO complaint -, hardly a validated method of detection. It is the complete opposite. Here you see the NIH themselves saying Lyme and LYMErix disease cause global immunosuppression with no antibodies but with chronic brain inflammation.
I repeat. This is not a bad knee and even SmithKline, the manufacturer of LYMErix, said Allen Steere was a nut. Publicly, and For The Record.
Finally, people should know the discoverer of Lyme disease said this about Allen Steere and his stupidometric, criminal testing schema:
Andy Wilson: “How do you feel about the controversy in the Lyme world?”
Dr. Burgdorfer: “The controversy in Lyme disease research is a shameful affair. And I say that because the whole thing is politically tainted. Money goes to people who have, for the past 30 years, produced the same thing—nothing. Serology has to be started over from scratch with people who dont know beforehand the results of their research.”
In other words, someone not involved in the Lyme disease cryme and scandal in the past should take a fresh look at what Lyme antibody profiles look like.
…………………………………………………………………………………………..
METHODS; Oy, why be current when the same old failed ideas continue to work terribly in the 21st Century. After all, the struggle for us is brainless “doctors” who would never dare to be seen without Kool-Aid stained lips and some who don’t know PubMed exists much less know how to use it.
<Well, actually THANKS, since this phenomenon helps us to understand the difference between stupid and ignorant. Stupid is willful or the product of arrogance.>
One develops and validates an analytical method first and foremost on the, generally speaking, accuracy, or the percentage of samples where the analyte (already known to be specific – or only detects one thing) is KNOWN to be present. “It should be 100%” the FDA told me on the phone (I knew that).
In a typical FDA assay development, Accuracy more refers to, for example, your method finding 98-102% of the analyte present in repeat samplings, when it is known to be present at 100% of the target concentration (say, such and such milligrams per liter). But in testing for the presence of antibodies to an infectious agent, the test you develop SHOULD CERTAINLY find all the cases – if not most, limited by the human subject only -, otherwise, there is no point. Right now Lyme testing finds only 15% of the cases, which was a criminal act. The patent owned by Yale (US 5,618,533) on Borrelia burgdorferi specific flagellin was 17/18 known cases detected, and it excluded flagellins from other organisms. That means it was 94.4% ACCURATE for detecting ALL cases of Lyme, not just HLA linked, late and early. It means this test was 100% SPECIFIC to burgdorferi because it EXCLUDED other organisms’ flagellins. Take a look at what they did:
Infect Immun. 1991 Oct;59(10):3531-5.
Molecular characterization of the humoral response to the 41-kilodalton flagellar antigen of Borrelia burgdorferi, the Lyme disease agent.
Berland R1, Fikrig E, Rahn D, Hardin J, Flavell RA.
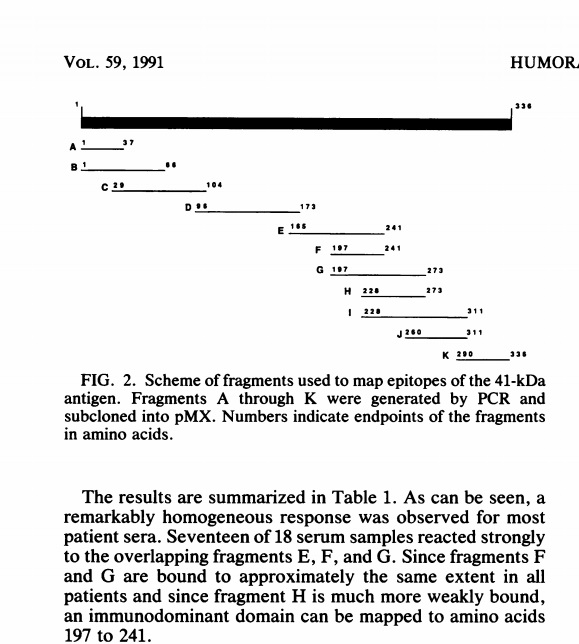
The earliest humoral response in patients infected with Borrelia burgdorferi, the agent of Lyme disease, is directed against the spirochete’s 41-kDa flagellar antigen. In order to map the epitopes recognized on this antigen, 11 overlapping fragments spanning the flagellin gene were cloned by polymerase chain reaction and inserted into an Escherichia coli expression vector which directed their expression as fusion proteins containing glutathione S-transferase at the N terminus and a flagellin fragment at the C terminus. Affinity-purified fusion proteins were assayed for reactivity on Western blots (immunoblots) with sera from patients with late-stage Lyme disease. The same immunodominant domain was bound by sera from 17 of 18 patients. This domain (comprising amino acids 197 to 241) does not share significant homology with other bacterial flagellins and therefore may be useful in serological testing for Lyme disease.
https://www.ncbi.nlm.nih.gov/pubmed/1894359
Look closely at this graphic from the full text report:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC258917/pdf/iai00046-0199.pdf
They created fragments of the DNA for flagellin and then fragments of that protein to see if there was a SPECIFIC fragment of the flagellin protein against which only Lyme victims had antibodies. Very straightforward.
Allen Steere had said originally (before the fake vaccine idea came along, and of course before New York Medical College’s association with Kaiser-Permanente, that resulted in the ALDF.com in 1990):
J Clin Invest. 1986 Oct;78(4):934-9.
Antigens of Borrelia burgdorferi recognized during Lyme disease. Appearance of a new immunoglobulin M response and expansion of the immunoglobulin G response late in the illness.
Craft JE, Fischer DK, Shimamoto GT, Steere AC.
Abstract
Using immunoblots, we identified proteins of Borrelia burgdorferi bound by IgM and IgG antibodies during Lyme disease. In 12 patients with early disease alone, both the IgM and IgG responses were restricted primarily to a 41-kD antigen. This limited response disappeared within several months. In contrast, among six patients with prolonged illness, the IgM response to the 41-kD protein sometimes persisted for months to years, and late in the illness during arthritis, a new IgM response sometimes developed to a 34-kD component of the organism. The IgGresponse in these patients appeared in a characteristic sequential pattern over months to years to as many as 11 spirochetal antigens. The appearance of a new IgM response and the expansion of the IgG response late in the illness, and the lack of such responses in patients with early disease alone, suggest that B. burgdorferi remains alive throughout the illness.
https://www.ncbi.nlm.nih.gov/pubmed/3531237
And from the full text report:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC423723/pdf/jcinvest00109-0086.pdf
Steere is saying here that all you need is band 41 to diagnose Lyme and that it is the earliest antibody to show up. Other scientists came to the same conclusion in the late 1980s and early 1990s. Just use band 41. Make it specific to Lyme or use several specific fragments of flagellins from the rest of the common Borreliae. In the next paragraph, Steere says treatment fails in half the cases:

https://www.ncbi.nlm.nih.gov/pmc/articles/PMC423723/pdf/jcinvest00109-0086.pdf
In a proper validation, the Sensitivity of the test you are developing means the same thing as Limit of Lowest Quantitation, or LLOQ or “how low in analyte concentration can your test reliably (3-5 standard deviations above “baseline noise” or the signal of a blank) detect?”
In other words, the truth about a valid test is the complete opposite of what the Lyme criminals claim. (Alligators. Even a small bite is nasty because of all the germs they harbor in their mouths, after all.)
Now let’s take a look at the old-fashioned ELISA (first step in the ridiculous proposal such as to look for the highest concentration of the analyte in question, rather than the lowest):
Enzyme-Linked Immunosorbent Assay (ELISA) – Multi-Lingual Captions
That is about the clunkiest test – so many steps – anyone could have ever devised, not to mention the concept is wrong. What if we were looking for early EBOLA or something.
Now look at the procedure for Western Blotting (OMG yer gonna be pulling your hair out at the steps and the waste of time):
https://www.youtube.com/watch?v=VgAuZ6dBOfs
AND MEANWHILE… some examples of new methods of detection (between “10-” and “22 times more sensitive than an ELISA” at detecting antibodies, among them):
— A nanotech method that we would run in the reverse: use flagellar antigen and try to capture anti-flagellin antibodies, known to be the only antibody present in the majority of the cases of Lyme detection (see US Patent 5,618,533 since that is a validation):
InnovaCoat® GOLD – gold nanoparticle conjugation
https://www.youtube.com/watch?v=FuhoIdE23mw
— Another (ironically, the US Navy, where Edward McSweegan used to NOT work in a lab before his fake whistleblower letter to Senator Barry Goldwater which was an attempt to steal the Navy’s funding for vector borne diseases research and give that funding to his cronies at the ALDF.com) :
https://frtr.gov/pdf/meetings/dec04/murday_12-04.pdf
Analyst. 2017 Sep 21. doi: 10.1039/c7an01231d. [Epub ahead of print]
Enhanced anodic electrochemiluminescence of CdTe quantum dots based on electrocatalytic oxidation of a co-reactant by dendrimer-encapsulated Pt nanoparticles and its application for sandwiched immunoassays.
Ren LL1, Dong H1, Han TT1, Chen Y2, Ding SN1.
Herein, we synthesized Pt dendrimer-encapsulated nanoparticles (Pt DENs) using amine-terminated sixth-generation polyamidoamine dendrimers. The enhanced and stable anodic electrochemiluminescence (ECL) of 3-mercaptopropionic acid-capped CdTe quantum dots (QDs) in a tripropylamine solution was achieved owing to Pt DENs. The reason may be that Pt DENs exhibit high catalytic electrochemical oxidation in the presence of tripropylamine and excellent conductive property. Inspired by this, Pt DENs were conjugated with Fe3O4@SiO2nanoparticles and served as nano-carriers. The capture antibodies were immobilized on the Fe3O4@SiO2-Pt DEN nanocomposites, which possess many attractive advantages such as the ease of bioconjugation, large specific surface area, and convenience of magnetic separation. Fluorescence microscopy images and UV-vis spectra were used to verify the immobilization of capture antibodies on the nanocomposites. The CdTe QDs were applied as signal labels for conjugation of nanocomposites with detection antibodies, which were characterized by agarose gel electrophoresis. Electrochemical impedance spectroscopy and cyclic voltammetry demonstrated the successful preparation of an ECL immunosensor. Under the optimal conditions, the proposed immunosensor provided a wide linear range from 0.005 ng mL-1 to 150 ng mL-1 with a detection limit of 0.2 pg mL-1 (S/N = 3) for the detection of carcinoembryonic antigen. Moreover, the immunosensor showed good performance for the detection of carcinoembryonic antigen in serum samples as well as great potential in clinical bioassay.
https://www.ncbi.nlm.nih.gov/pubmed/28932837
Biosens Bioelectron. 2017 Mar 15;89(Pt 1):370-376. doi: 10.1016/j.bios.2016.06.073. Epub 2016 Jun 25.
Carboxyl-functionalized graphene oxide composites as SPR biosensors with enhanced sensitivity for immunoaffinity detection.
Chiu NF1, Fan SY2, Yang CD2, Huang TY2.
This work demonstrates the excellent potential of carboxyl-functionalized graphene oxide (GO-COOH) composites to form biocompatible surfaces on sensing films for use in surface plasmon resonance (SPR)-based immunoaffinity biosensors. Carboxyl-functionalization of graphene carbon can modulate its visible spectrum, and can therefore be used to improve and control the plasmonic coupling mechanism. The binding properties of the molecules between a sensing film and a protein were elucidated at various flow rates of those molecules. The bio-specific binding interaction among the molecules was investigated by performing an antigen and antibody affinity immunoassay. The results thus obtained revealed that the overall affinity binding value, KA, of the Au/GO-COOH chip can be significantly enhanced by up to ∼5.15 times that of the Au/GO chip. With respect to the shifts of the SPR angles of the chips, the affinity immunoassay interaction at a BSA concentration of 1μg/ml for an Au/GO-COOH chip, an Au/GO chip and a traditional SPR chip are 35.5m°, 9.128m° and 8.816m°, respectively. The enhancement of the antigen-antibody interaction of the Au/GO-COOH chip cause this chip to become four times as sensitive to the SPR angle shift and to have the lowest antibody detection limit of 0.01pg/ml. These results indicate the potential of the chip in detecting specific proteins, and the development of real-time in vivo blood analysis and diagnosis based on cancer tumor markers.
https://www.ncbi.nlm.nih.gov/pubmed/27396822
Expert Rev Clin Immunol. 2013 Mar;9(3):263-80. doi: 10.1586/eci.12.110.
Leptospirosis: current situation and trends of specific laboratory tests.
Schreier S1, Doungchawee G, Chadsuthi S, Triampo D, Triampo W.
Leptospirosis is re-emerging as a worldwide zoonosis and is caused by bacteria of the genus Leptospira. Human leptospirosis is associated with high temperature and humidity. Laboratory tests are indispensible for the early diagnosis and proper disease management. The demand for suitable leptospirosis point-of-care diagnostic tests grows with the awareness and number of incidences. Confirmation is achieved by the microscopic agglutination test, bacterial cultivation, PCR or histopathologic methods. However, high costs, poor standardization and/or elaborate sample preparation prevent routine use at the point of care. Cost-efficient, but insensitive serological methods dominate the diagnostic landscape and, likewise, urgently need improvement toward greater compliance with some of the point-of-care criteria. Combined application of antigen and antibody detection methods increases accuracy, but also new development or transfer of diagnostic technologies should be considered useful. Nano- and microparticle technology may play a key role in improving future antigen detection methods.
https://www.ncbi.nlm.nih.gov/pubmed/23445200
And about 800 reports where we see “10” to “22” times more sensitive than an ELISA:
https://www.ncbi.nlm.nih.gov/pubmed/?term=nano*+and+(%22antibody+detection%22+or+immunoassay)
AND, the patent database:
http://patft.uspto.gov/netacgi/nph-Parser?Sect1=PTO2&Sect2=HITOFF&p=1&u=%2Fnetahtml%2FPTO%2Fsearch-bool.html&r=0&f=S&l=50&TERM1=nanosensor&FIELD1=&co1=AND&TERM2=antibodies&FIELD2=&d=PTXT
Here is an interesting patent:
“Magnetic separation and a nanosensor are used to improve the signal-to-noise ratio for measuring analyte levels 1,000,000 times lower than enzyme-linked immunosorbent assay (ELISA).”
http://patft.uspto.gov/netacgi/nph-Parser?Sect1=PTO1&Sect2=HITOFF&d=PALL&p=1&u=%2Fnetahtml%2FPTO%2Fsrchnum.htm&r=1&f=G&l=50&s1=9,624,532.PN.&OS=PN/9,624,532&RS=PN/9,624,532
A million times more sensitive than an ELISA for detecting antibodies. Hmm. Might be an idea.
.
Well, the problem really is, “What do we do with these patients once we find out it was Borrelia that caused the “sepsis induced immunosuppression” or the Great Imitators?”
Once again, we propose it will be sciencey. And will use really, really sciencey words. It won’t have anything to do with eye of newt or juice of carrot or this or that hocus pocus Oil of Whatever. It wont be stray electrons or onion socks. It CERTAINLY wont be antibiotics if Lyme is well known to cause cancer, MS, and Lupus.
If LYMErix caused the same sepsis-induced immunosuppression (that’s a formal term now, use either your Google or PubMed Machine) as Lyme itself, if Lyme causes a pseudolymphoma and/or deformed B cells, … then let’s be wild and over-the-top and unconventional and propose the treatment should address the tolerance and cross tolerance, as well as the “EBV-like – transformed lymphocytes.”
The problem (and the prosecution-solution) starts with the testing. But these crazy assholes (SmithKline and Burgdorfer both think Allen Steere is crazy and incompetent) said we were, for the sake of their Beloved ALDF “Vaccines and Test Kits DNA Empire.”
They’ll never live this down and neither will the “LLMDs” and the other charlatans of Lyme.
_________________________________________________
____________________________________________________________
………………………………………………………………………………………………………………..
ABOUT THE TESTING VS THE DISEASE:
FIRST, The ALDF.com Cabal (McSweegan circa 1986 – this needs to be made into a pdf):
http://www.actionlyme.org/GOLDWATER_LETTER.htm
.
Bayh-Dole Act:
https://en.wikipedia.org/wiki/Bayh%E2%80%93Dole_Act
Patents of Damocles – an article about fraudulent patent enforcement, which is part of the RICO charge with “Deprivation of Rights Under Color of Law”
http://www.repository.law.indiana.edu/ilj/vol83/iss1/4/
It should be a criminal charge, says this man, Christopher Leslie.
– – – –
THE DC- TC PRESENTATION (2017):
https://docs.wixstatic.com/ugd/47b066_85956946d37c44d8bee5ba73d43ee5ac.pdf
THE CRIMINAL CHARGES AS THEY WERE BEFORE WE REFINISHED THE CHARGE SHEETS (needs to be updated)
http://www.actionlyme.org/170308_SASH_LOBBY_BOOKLET.pdf
DEARBORN BOOKLET
http://www.actionlyme.org/DEARBORN_PDF.pdf
DEARBORN INVITATION – this shows it was a consensus conference and no one agreed, in the end, as the Dearborn booklet shows:
http://www.actionlyme.org/DEARBORNINVITATION.pdf
STEERE FALSIFIES THE TESTING – THE REPORT NOT INCLUDED IN THE DEARBORN BOOKLET:
http://www.actionlyme.org/dressler1994.pdf
DURAY AND STEERE, 1988, LYMPHOMA
http://www.actionlyme.org/clinical-pathologic-correlations-of-lyme-disease-by-stage-Steere-Duray.pdf
DURAY, 1989, IDSA’s “Reviews” (needs to me made into a pdf)
http://www.actionlyme.org/IDSA_CLINIPATH_DURAY.htm
DATTWYLER SAYING BORRELIAL SUPERNATANTS (insoluble Osps) CAUSE IMMUNOSUPPRESSION:
http://www.actionlyme.org/golightly_Datt1988.pdf
DATTWYLER’S SERONEGATIVE LYME ASSAY:
http://www.actionlyme.org/dattwyler1988_1.pdf
STEERE, 1990, and “CHRONIC NEUROLOGIC LYME” where he uses Dattwyler’s Seronegative Lyme Assay:
http://www.nejm.org/doi/pdf/10.1056/NEJM199011223232102
STEERE in 1991 “Rheumatology News,” saying Lyme causes everything including seronegative Lyme and CFIDS (same thing – post Lyme sepsis):
https://groups.google.com/forum/#!original/sci.med.diseases.lyme/UwAp8BhxwAU/R9-e2JQGN1AJ
DURAY and STEERE in SCHUTZER’s 1992 BOOK and the ALDF’s “Lyme Disease” book, from 1998, (Steere admits you are only seropositive if you have arthritis)

1998: – the Munchausen’s Book:

Who Says OspA causes Immunosuppression (From the Razor) – and/or Causes Lymphoma or Pseudolymphoma:
LUFT at the FDA, 1998 (SmithKline and Yale threw out nearly 1000 cases of severe Lyme like adverse events – it is admitted here):
https://www.fda.gov/ohrms/dockets/ac/98/transcpt/3422t1.rtf
“The point that I wanted to make in regard to the study is that there is very heavy dependence on serologic confirmation. And when we start thinking about the adverse events, it was stated originally when we got the overview of the disease that the disease is really quite protean. And actually the adverse events are very similar to what the disease manifestations are. And if you start to, as I think Dr. Hall was eluding to — if you start to kind of say well how often do you actually become sero positive, you can start to have a different take on when someone has an adverse event of whether it is disease specific or infection specific versus vaccine specific. And I think that that is an important issue that we have to deal with.”
Luft at the FDA, 2001; if you read this carefully you will see Luft is fighting these pricks the whole way over LYMErix as a “vaccine”:
https://www.fda.gov/ohrms/dockets/ac/01/transcripts/3680t2.rtf
LUFT: It appears that from the data that you presented that there was no difference in the signs of symptoms in those patients who had, in other words, vaccine failure. And so that they probably — do you have a serologic correlate of that?
LUFT: In a way I feel like I’m almost in a twilight zone when we are talking about surveillance and these adverse events, and I forgot the name of the — one of the vice presidents from Smith Kline.
What disturbs me is that in the SmithKline presentation there were 950 adverse events. There was a nice presentation of that. And this afternoon we heard testimony from 20 individuals of 20, of approximately 20 people who had very significant adverse events.
And the disconnect for me is I’m hearing that, and I’m seeing that data, and I don’t see any reflection of one to the other as if we were in two different universes.
I’m not ascribing what the validity is to these complaints. Certainly I was moved by it. But the fact of the matter that it didn’t even enter into the discussion, or into the charts, or the tables, is disturbing.
Reference;https://crymedisease.wordpress.com/2017/09/22/the-analytics-of-lyme-disease/